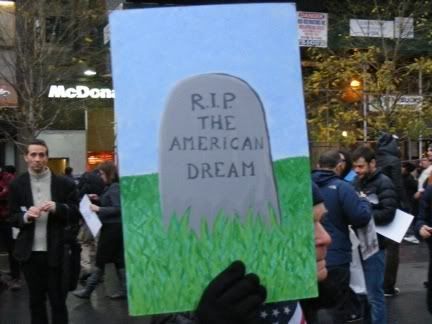
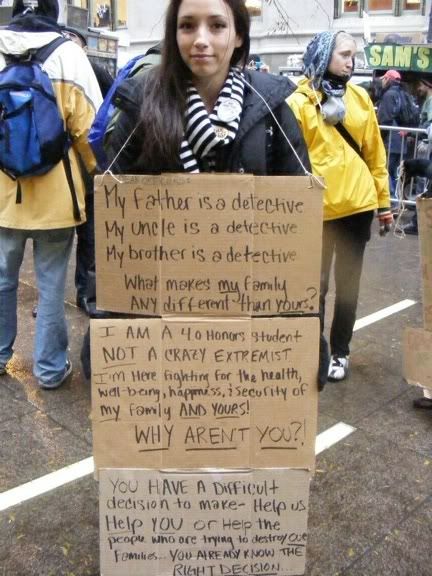
Protester at Union Square, November 17, 2011. Photo: Edward Arrocha.
One thing that's been on my mind over the past few weeks is the question often repeated on the news and in the media: what is OWS asking for? Granted, there is a detailed
OWS declaration outlining "a feeling of mass injustice" thanks to a "corrupted system" that includes inequality and discrimination; environmental destruction and oil dependence; corporate control of the media, the courts, the government, and the economy; bank bailouts, executive bonuses at taxpayer expense, and improper seizure of homes during the mortgage crisis; lack of regulation of campaign finance; the right to education, privacy, and health care; and more. I've seen OWS summed up as "Corporate Greed is killing the American Dream" and many more nice, short messages that fit neatly on a signboard.
But at the heart of it, there is a focus on individual people and their own stories. I've heard it said again and again, "We all have a story." OWS includes the unemployed, underemployed, uninsured, and financially overextended, but it also includes many who are simply deeply concerned that our democratic system is broken and no longer provides equally for all of its citizens. I think, for the most part, people want jobs for fair wages; they want food (dare I say healthy food!), clothing, and shelter; they want health care for themselves and their families.
Frightening
new statistics from the the U.S. Census Bureau place "100 million people — one in three Americans — either in poverty or in the fretful zone just above it." There are many who like to portray those on public assistance as lazy and undeserving of help and bemoan throwing their tax money into a "welfare state."
The article goes on to point out, however, that
"of the 51 million who appear near poor under the fuller measure, nearly 20 percent were lifted up from poverty by benefits the official count overlooks. But more than half were pushed down from higher income levels [emphasis mine]: more than eight million by taxes, six million by medical expenses, and four million by work expenses like transportation and child care." In other words, more than half of the 51 million Americans in this borderline-poverty category got there by doing the right thing: paying their taxes responsibly and taking care of themselves and their families by paying for health care, going to and from work, and paying for child care.
Protester at Union Square, November 17, 2011. Photo: Edward Arrocha.
As for Medicare and Social Security, there have been no cost-of-living increases to Social Security since 2009. 55 million Americans depend on this income to pay for their homes, food, and other necessities. Medicare allows them to pay for medication and the health care they need to live. The idea of cutting these programs is absurd -- Social Security benefits represent about 41% of the income of the elderly. And before Medicare was enacted in 1965, just 56 percent of seniors had hospital insurance. We--all taxpayers and all workers--pay into these programs. Cutting them will result in more homelessness, hunger, poverty, and needless suffering in the streets and public emergency rooms--resulting in more taxes and even higher insurance premiums.
As one example of what people are looking for in their lives, I turn to health care and how badly people want--need--health insurance.
 Disaster Relief Medicaid was available to New York City residents from September 2001 through January 2002. Participants received four months of coverage through traditional Medicaid providers.
Disaster Relief Medicaid was available to New York City residents from September 2001 through January 2002. Participants received four months of coverage through traditional Medicaid providers.
Squad Company 18 Firehouse shortly after September 11, 2001. Photo: Chris Clarke
The article illustrated one crucial point to me -- officials making policy are pathetically out of touch with their consituents and what they need. It was no surprise to me that people who work--often 60 to 70 hours a week--have no health insurance, as this was true of most of my friends. It also was not news to me that people want to get glasses, go to the dentist, and have regular medical check-ups.
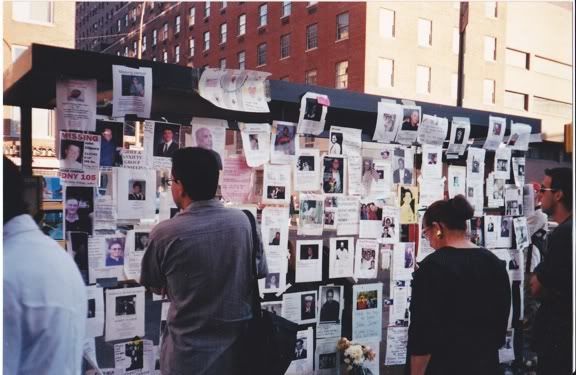
Wall of posters searching for people missing after September 11, 2001. Photo: Chris Clarke
According to New York State's report on the DRM, the program was implemented by mandate from Governor Pataki about two weeks after 9/11 with a "streamlined" application process. "Infrastructure-supported communication with Medicaid computer systems suffered severe damage. Public transportation was disrupted. Information necessary to establish eligibility was not readily available. Faced with the likelihood of increased health care needs, and the inability to conduct business as usual...a new, time-limited program called Disaster Relief Medicaid/Family Health Plus [was created]. ... The DRM program was unprecedented, and so was enrollment. Thousands of New Yorkers signed up between September 2001 and January 2002. Thus DRM became an unintentional laboratory for examining the consequences of a radically simplified approach to government-funded health care." [P. 5] Mr. O'Kitten was among the 342,362 New Yorkers who enrolled. [P. 21]
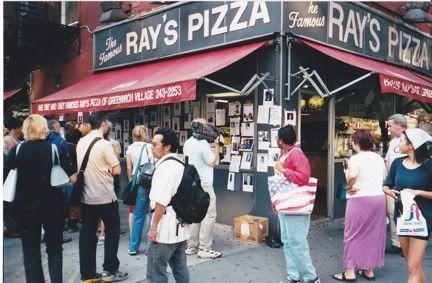
Ray's Pizza in the West Village papered with posters searching
for people missing after September 11, 2001. Photo: Chris Clarke.
Unlike the traditional Medicaid application, DRM allowed you to have higher income ($716/month for individuals, $968/couples) and the only requirements (besides income) were that you be a NYC resident with a Social Security number. The application itself was reduced from 8 pages (plus supporting documents, like bank statements and pay stubs) to a single page. Approval was reduced to 1-5 days from 1-3 months. [P. 13]
Interestingly and importantly, "Providers reported discovering a number of early cancers, early-onset heart disease, and previously undetected diseases such as diabetes, asthma, and HIV among DRM recipients." And how much of a savings in actual dollars (not to mention prevented suffering) does such early detection represent? [p.7]
Lower Manhattan shortly after September 11, 2001. Photo: Chris Clarke.
Here's the report's documentation for the DRM enrollees' use of eye care and dental services: "Generally, utilization of Medicaid services by DRM enrollees was consistent with the regular Medicaid population. Exceptions were Dental ($125 million), Laboratory ($4 million), and Eye Care Services ($5.8 million), which were utilized at higher rates; and Inpatient Services ($194 million), which were utilized at a lower rate." [p.7] "More than 9,000 individuals [2.7%] utilized an inpatient service." [P. 15] Notably, "Nearly 23 percent of hospital admissions were for drug and alcohol treatment." [P. 15] Also of note, "More than 19,000 women sought treatment for gynecology services." [P. 15]
So what happened to DRM? "DRM was originally intended to provide four months of health care coverage. As the program evolved, it was decided to give DRM enrollees the opportunity to obtain regular Medicaid without a gap in coverage. This opportunity became the Transition Program. Following the four-month DRM authorizations, most enrollees (about 90 percent) were granted extensions, during which they could file a full application for regular Medicaid/Family Health Plus." [P. 21] "As of February 2003, there were 150,676 DRM enrollees, or 44.3 percent, who were ultimately transitioned to regular Medicaid or Family Health Plus from DRM." [P. 22]
The report notes a few interesting things in its conclusions. For instance, "The interviews and focus groups confirmed that, for some people, the life circumstances that create the need for Medicaid often prevent people from obtaining the documentation required to prove eligibility." [P. 48] Any illness that affects physical mobility would certainly fall into just such a life circumstance, as would mental illness. It would also be difficult for someone juggling many hours of low-wage work and child care to spend a day filing for Medicaid. You have file in person (which means taking the day off of work and finding a babysitter) and you may be required to return if you don't have all the proper documentation with you, which is almost a given since they always seem to come up with something you didn't bring with you.

Marylanders seeking help flood the Baltimore County office
of the State Department of Social Services. Photo: Frank Klein
For a glimpse at how daunting the application itself is, you can look at it here. As for the required documentation, the DRM report points out, "Some individuals, primarily those who work “off the books,” have problems in documenting employment. Others who have difficulty include seasonal workers whose previous year’s returns may not reflect their current situation, workers with a variety of temporary jobs, and self-employed individuals with irregular income for multiple services. It also appears that the types of employment that do not offer health insurance are often the most difficult to document." [P. 48-49]
"[DRM] Participants’ health status varied considerably. Many of the participants felt they were in relatively good health and needed only routine preventive examinations. They had often lived with dental problems, allergies, and chronic pain without receiving treatment except in emergencies. About ten percent of the participants had chronic health conditions such as diabetes, lupus, high blood pressure, and cancer that require ongoing care. Many stated they would do “whatever they could” to purchase the medications and treatments as often as possible. Their economic situation did not allow them to have the kind of health care their medical situation warranted [emphasis mine]. Each focus group had one or two elderly participants with at least one, and often multiple, serious, chronic health care problems. They could not afford to purchase the medications and treatments that were not fully covered by Medicare (even if they were enrolled)." [P. A-8]

"The many reasons for applying for DRM reflected participantsʼ diverse health needs. Many participants used DRM for preventive services such as check-ups, mammograms, pap smears, prostate exams, and lab tests. Dental services was mentioned most often. Receiving vision care was also a commonly used service. One participant saw a psychiatrist to help him with his reaction to 9/11. Those with previously diagnosed chronic health problems often enrolled to receive care they could not always afford in the past, including medications. Many said they signed up to receive health care services they knew they needed but could not afford [emphasis mine]. A number of individuals had relied on emergency room visits for treatment in the past." [P. A-8, 9]"We hold these truths to be self-evident, that all men are created equal, that they are endowed by their Creator with certain unalienable Rights, that among these are Life, Liberty and the pursuit of Happiness.--That to secure these rights, Governments are instituted among Men, deriving their just powers from the consent of the governed, --That whenever any Form of Government becomes destructive of these ends, it is the Right of the People to alter or to abolish it, and to institute new Government, laying its foundation on such principles and organizing its powers in such form, as to them shall seem most likely to effect their Safety and Happiness. Prudence, indeed, will dictate that Governments long established should not be changed for light and transient causes; and accordingly all experience hath shewn, that mankind are more disposed to suffer, while evils are sufferable, than to right themselves by abolishing the forms to which they are accustomed." [The
Declaration of Independence, July 4, 1776.]
If we are indeed a First World country, and believe in Life, Liberty, and the pursuit of Happiness, it is indeed shameful that any one of us should endure ill health when modern medicine can relieve us of our suffering.
“Does it make you a king
to have more and more cedar?
Did not your father have food and drink?
He did what was right and just,
so all went well with him.
He defended the cause of the poor and needy,
and so all went well.
Is that not what it means to know me?”
declares the LORD.
“But your eyes and your heart
are set only on dishonest gain,
on shedding innocent blood
and on oppression and extortion.”
Therefore this is what the LORD says about Jehoiakim son of Josiah king of Judah:
“They will not mourn for him:
‘Alas, my brother! Alas, my sister!’
They will not mourn for him:
‘Alas, my master! Alas, his splendor!’
He will have the burial of a donkey—
dragged away and thrown
outside the gates of Jerusalem."
Jeremiah 22:15-19
Protester at Union Square, November 17, 2011. Photo: Edward Arrocha.








{kind=link}
1 comment:
I really don't think they're going to solve the health care crisis until they divorce it from employment.
That application doesn't look too arduous to me but mind you, I worked for Kaiser for 20 years.
Post a Comment